
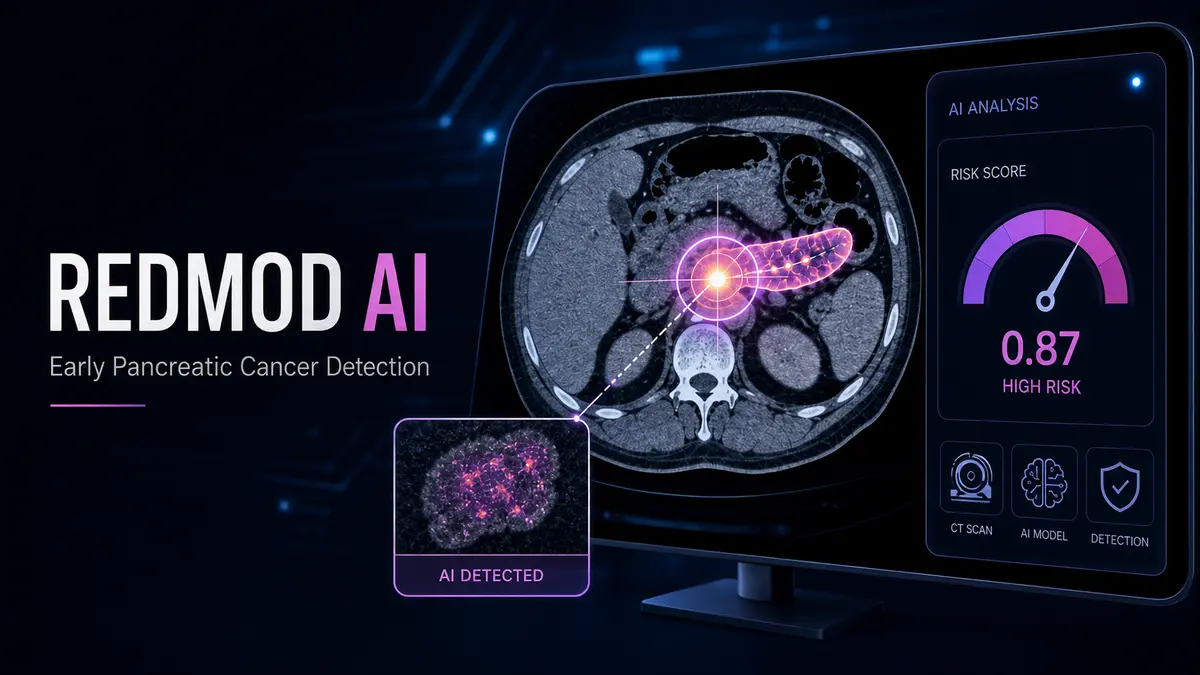
REDMOD, an AI radiomics model, may help detect subtle signs of pancreatic cancer in routine CT scans before tumors become clearly visible. The development highlights how artificial intelligence could support earlier diagnosis, better clinical decision-making, and a new future for cancer detection.
Pancreatic cancer has long been one of the most feared diseases in modern medicine. Not because it is the most common cancer, but because it is often discovered too late.
By the time many patients develop symptoms, the disease may already have advanced beyond the stage where surgery or curative treatment is possible. This harsh clinical reality has made early detection one of the most urgent challenges in oncology.
Now, artificial intelligence may be opening a new window. A recently reported AI system called REDMOD, short for Radiomics-based Early Detection Model, has shown the ability to detect early signs of pancreatic cancer in CT scans before tumors become clearly visible to human experts. The model was developed and validated by researchers from Mayo Clinic and collaborating institutions, with the study published in Gut, a leading medical journal.
REDMOD is designed to identify visually occult pancreatic ductal adenocarcinoma, meaning cancer signals that are present in imaging data but not obvious to the radiologist’s eye. The finding is significant because pancreatic cancer is not merely a treatment problem. It is also a timing problem. Medicine often finds the disease after it has already gained the advantage. REDMOD suggests a different future: one where AI does not replace doctors, but helps them see risk earlier.
Why Pancreatic Cancer Is So Difficult to Detect
Pancreatic cancer is difficult because it hides well. The pancreas sits deep inside the abdomen, behind the stomach. Small tumors can grow without causing clear symptoms. Early warning signs, when they appear, may be vague: fatigue, weight loss, digestive discomfort, abdominal pain, back pain, jaundice, or new-onset diabetes. These symptoms can be caused by many other conditions, so the cancer is often not suspected immediately.
This delay matters.
According to American Cancer Society data, the five-year relative survival rate for pancreatic cancer remains around 13% across all stages combined. The survival rate is much higher when the disease is localized, but drops sharply when the cancer has spread. Localized pancreatic cancer has a reported five-year relative survival rate of about 44%, while distant-stage disease has a survival rate of only around 3%.
That gap explains why early detection is so important. If the disease is discovered before it spreads, doctors may have more options. Surgery, chemotherapy, radiation, and emerging targeted therapies become more meaningful when the cancer is caught early. But today, most patients are not diagnosed at that ideal moment. This is where AI-assisted imaging could become important.
What Is REDMOD?
REDMOD stands for Radiomics-based Early Detection Model.
Radiomics is a field that extracts large amounts of quantitative information from medical images. A CT scan is not treated only as a picture. It becomes a structured data source. Pixel intensities, tissue texture, shape, density, spatial variation, and subtle imaging patterns can be converted into measurable features.
A radiologist may look at a scan and see a pancreas that appears normal. A radiomics model may detect small changes in tissue structure that are not visually obvious. REDMOD uses this principle to analyze CT scans and identify early tissue patterns associated with pancreatic ductal adenocarcinoma, the most common form of pancreatic cancer. The model is not looking for a large visible tumor in the traditional sense. Instead, it is searching for hidden signals that may appear before clinical diagnosis.
Mayo Clinic reported that REDMOD identified 73% of prediagnostic cancers at a median of around 16 months before diagnosis. In scans taken more than two years before diagnosis, the AI identified nearly three times as many early cancers compared with unaided expert review.
That does not mean REDMOD is ready to become a universal screening tool tomorrow. It does mean the research points toward a powerful new direction. The real breakthrough is not simply that AI can read scans. The breakthrough is that AI may be able to detect disease patterns before humans know what to look for.
From Visible Disease to Hidden Risk
Traditional medical imaging is built around visibility. A doctor orders a scan. A radiologist examines the image. If a lesion, mass, duct change, or abnormal structure is visible, it may trigger further investigation. This process has served medicine for decades and remains essential. But the limitation is clear. If the disease is not yet visible, the scan may be reported as normal. REDMOD challenges that boundary. Instead of asking, “Is there a visible tumor?” the model asks a more technical question: “Are there subtle imaging features that resemble the early biological footprint of pancreatic cancer?”
This is an important shift. AI models can process high-dimensional patterns across thousands of imaging features. They do not become tired. They do not rely only on visual memory. They can compare microscopic differences in texture, density, and tissue structure across large datasets. That makes them useful for diseases where early signs are too faint, too distributed, or too complex for consistent human detection. In simple words, REDMOD may help convert a normal-looking CT scan into a risk signal.
Why CT Scans Matter
One of the most interesting aspects of REDMOD is its focus on routine CT imaging. Many patients receive abdominal CT scans for reasons unrelated to cancer: stomach pain, kidney stones, trauma, digestive problems, or other abdominal complaints. In some cases, those scans may contain early pancreatic changes even before cancer is diagnosed. If AI can analyze existing scans more deeply, hospitals may be able to identify high-risk patients without always needing an entirely new screening infrastructure. This matters for scalability.
A new blood test or specialized scan may require separate adoption, reimbursement, and clinical workflows. But CT scans are already part of modern healthcare. If AI can run quietly in the background and flag suspicious patterns, it could become a second layer of intelligence on top of existing radiology systems. That is the larger promise of medical AI: not replacing the hospital, but upgrading the intelligence inside it.
AI Will Not Replace Radiologists
This point must be stated clearly. REDMOD is not a replacement for radiologists, oncologists, gastroenterologists, surgeons, or clinical judgment. It is a decision-support system.
In medicine, a false alarm is not a small matter. If an AI model wrongly flags a patient as high-risk, it may lead to anxiety, repeat imaging, biopsies, invasive procedures, or unnecessary specialist referrals. On the other hand, if the model misses a real case, the consequences may also be serious. That is why AI in healthcare must be judged differently from AI in consumer software. A chatbot can make a mistake and still be corrected. A medical AI system must work within evidence, regulation, clinical validation, patient safety, and physician oversight.
The correct future is not “AI versus doctors.” The correct future is AI-assisted doctors. In that model, REDMOD could serve as a risk detector. It flags scans that deserve a second look. The physician then decides whether the patient needs follow-up imaging, blood tests, specialist consultation, or watchful monitoring. This is how trustworthy AI enters medicine: not through theatrical replacement, but through disciplined assistance.
The Bigger Trend: Predictive Healthcare
REDMOD belongs to a much larger movement in healthcare AI. For years, medicine has mostly been reactive. A patient develops symptoms. The doctor investigates. The diagnosis follows. Treatment begins. But AI is pushing healthcare toward prediction.
Instead of waiting for disease to become obvious, AI systems may help identify risk earlier by combining imaging, biomarkers, genetics, electronic health records, pathology data, and patient history. This is especially relevant for diseases like pancreatic cancer, lung cancer, cardiovascular disease, Alzheimer’s disease, and certain rare disorders.
The technical foundation is multimodal intelligence. In the future, a cancer detection system may not rely only on a CT scan. It may combine radiomics, lab values, family history, genetic predisposition, new-onset diabetes patterns, weight loss signals, inflammation markers, and longitudinal imaging changes. That is where AI becomes more than image recognition. It becomes a clinical pattern engine. REDMOD is important because it shows how this future may begin: with one hard disease, one imaging modality, and one carefully validated model.
The Clinical Promise
If REDMOD or similar AI systems prove reliable in broader clinical settings, the impact could be meaningful. First, high-risk patients could be identified earlier. People with family history, genetic risk, chronic pancreatitis, or suspicious metabolic changes may benefit from closer monitoring. Second, radiologists could gain a second layer of support. Even experienced specialists may miss subtle signals when the pancreas appears normal. AI can provide another checkpoint.
Third, hospitals could build earlier intervention pathways. A flagged scan may trigger follow-up MRI, endoscopic ultrasound, tumor marker testing, or repeat imaging after a defined period. Fourth, cancer research itself could improve. If AI can identify prediagnostic imaging patterns, researchers may better understand how pancreatic cancer develops before it becomes visible. This is not only a diagnostic opportunity. It is a scientific opportunity.
The Risks and Open Questions
The excitement around REDMOD should be balanced with caution. Medical AI has a history of impressive research results that do not always translate smoothly into real-world hospitals. Data quality varies. Patient populations differ. Scanners are not identical. Imaging protocols change. A model trained in one environment may perform differently in another. External validation is therefore crucial.
The Gut study describes REDMOD as externally validated and longitudinally stable, which is encouraging. But before such a system becomes routine, it will need broader testing across different hospitals, countries, age groups, ethnic populations, scanner types, and clinical workflows. There are also ethical issues.
Who gets screened? Who owns the imaging data? How should patients be informed if an AI model detects risk but no visible tumor exists? What is the right follow-up plan? How should hospitals prevent unnecessary procedures while still acting early enough? These are not small questions. The power to detect risk before disease is visible must be matched with responsibility. Early detection is valuable only when it leads to better outcomes, not just more fear.
Why This Moment Matters
The REDMOD story comes at a time when AI is moving deeper into serious scientific and medical domains. The first wave of generative AI was dominated by text, images, chatbots, and productivity tools. The next wave may be different. It may focus on biology, diagnostics, drug discovery, clinical decision support, and personalized medicine.
This is where AI becomes less visible to the public but more important to human life. In consumer AI, the question is often whether the model can write, summarize, code, or generate media. In medical AI, the question is sharper: can the model help doctors act earlier, more accurately, and with greater confidence?
REDMOD is a reminder that the most meaningful AI systems may not look flashy. They may sit quietly inside hospitals, scanning medical images, finding hidden signals, and giving clinicians more time. And in pancreatic cancer, time is everything.
The Future Is Earlier, Not Just Smarter
REDMOD does not cure pancreatic cancer. It does not remove the need for doctors. It does not eliminate the uncertainty of medical diagnosis. But it points toward a future where cancer detection becomes earlier, deeper, and more data-driven.
For a disease like pancreatic cancer, that matters enormously. The tragedy of this cancer is not only its biological aggression. It is the fact that medicine often sees it after the best treatment window has begun to close. Artificial intelligence may help change that.
The most powerful role of AI in healthcare may not be replacing human expertise. It may be extending it. It may help doctors notice what was previously hidden, act before symptoms become obvious, and create a new diagnostic window where none existed before. The AI radiomics model is still a research milestone, not a universal hospital standard.
But its message is clear. The future of cancer detection may not begin when a tumor becomes visible. It may begin when AI detects the first faint signal that something is changing. And for patients facing one of the world’s deadliest cancers, that earlier signal could make all the difference.
Discover more from Poniak Times
Subscribe to get the latest posts sent to your email.





{kind=link}
{kind=link}